Audience
AI for residents and registrars: the workflows that buy back time in training
Updated 1 June 2026 · 11 min read
AI for residents and registrars is most valuable as a documentation, teaching and revision tool, not as a clinical decision aid. Used inside those jobs, free models like ChatGPT, Claude and NotebookLM cut prose tasks (reflections, logbook entries, journal-club summaries, teaching decks) by roughly 70 percent. Used outside them, the same tools breach GMC confidentiality guidance, miscalculate doses, and erode the supervised practice that training is supposed to build. This guide is the working stack, the time savings worth quoting, and the hard limits that keep you out of trouble at ARCP.
How to think about AI in postgraduate training
Residents, registrars and fellows have the opposite problem to medical students. The reading list is shorter, the unprotected hours are fewer, and the documentation load is heavier. AI's job in training is to compress the repetitive prose around clinical work so the limited supervised hours go to deliberate practice. Treat the model as a fast junior who drafts well, hallucinates occasionally, and must never sign anything.
The GMC's 2024 update to Good Medical Practice and the equivalent ACGME 2024 common program requirements both land in the same place: AI tools may support training, but the trainee remains the accountable clinician for every entry, every decision and every patient record. That accountability does not transfer to the model, the vendor, or your training programme director.
The five jobs worth automating in training
1. Logbook entries and case reflections
Draft eLogbook narratives, eportfolio reflections and ARCP CBDs from bullet-point notes. The Joint Committee on Surgical Training accepts AI-drafted logbook prose at ARCP from 2025 onward, provided the trainee personally verifies content and identifiers. ChatGPT or Claude will turn five bullet points into a 250-word reflection in under a minute. Read every line, fix any clinical drift, sign it yourself.
2. Teaching slide decks for juniors and medical students
Registrars teach. Gamma, Beautiful.ai and Canva's AI features turn a topic outline into a 12-slide teaching deck in about 90 seconds. They are excellent at structure and weak at medical imagery, so replace stock diagrams with figures from Radiopaedia, BMJ Best Practice or a sketch-first illustration tool. The deck stays yours; the AI absorbs the typesetting and layout.
3. Journal-club preparation
Upload the paper to NotebookLM. The free tier handles up to one million tokens of source material per notebook (Google, 2025), so RCTs, guidelines and Cochrane reviews all fit without trimming. Ask for population, intervention, primary outcome, secondary outcomes, key limitation and the strongest critique. Cross-check against the paper. You arrive at journal club with a pre-built skeleton and time for the actual argument.
4. Operative and procedural teaching diagrams
Drawing each step of a procedure is the fastest way to teach a junior how it goes. Generic text-to-image models still hallucinate surgical anatomy, so for teaching diagrams use a sketch-first tool such as Angiosome. Sketch the step on an iPad, render a clean labelled image in under a minute, build a teaching set for an entire procedure in roughly 20 minutes. The topology comes from you; the rendering comes from the model.
5. Exam revision (MRCP, MRCS, FRCA, FRCR, USMLE Step 3, ABIM)
Use ChatGPT or Claude for explanation and viva rehearsal, NotebookLM for grounded guideline review, and Anki with FSRS for retention. The stack is the same as medical school; the volume per topic is lower and the bar for clinical reasoning is higher. Pair AI explanations with a question bank (Passmedicine, eMRCS, UWorld) for actual exam calibration.
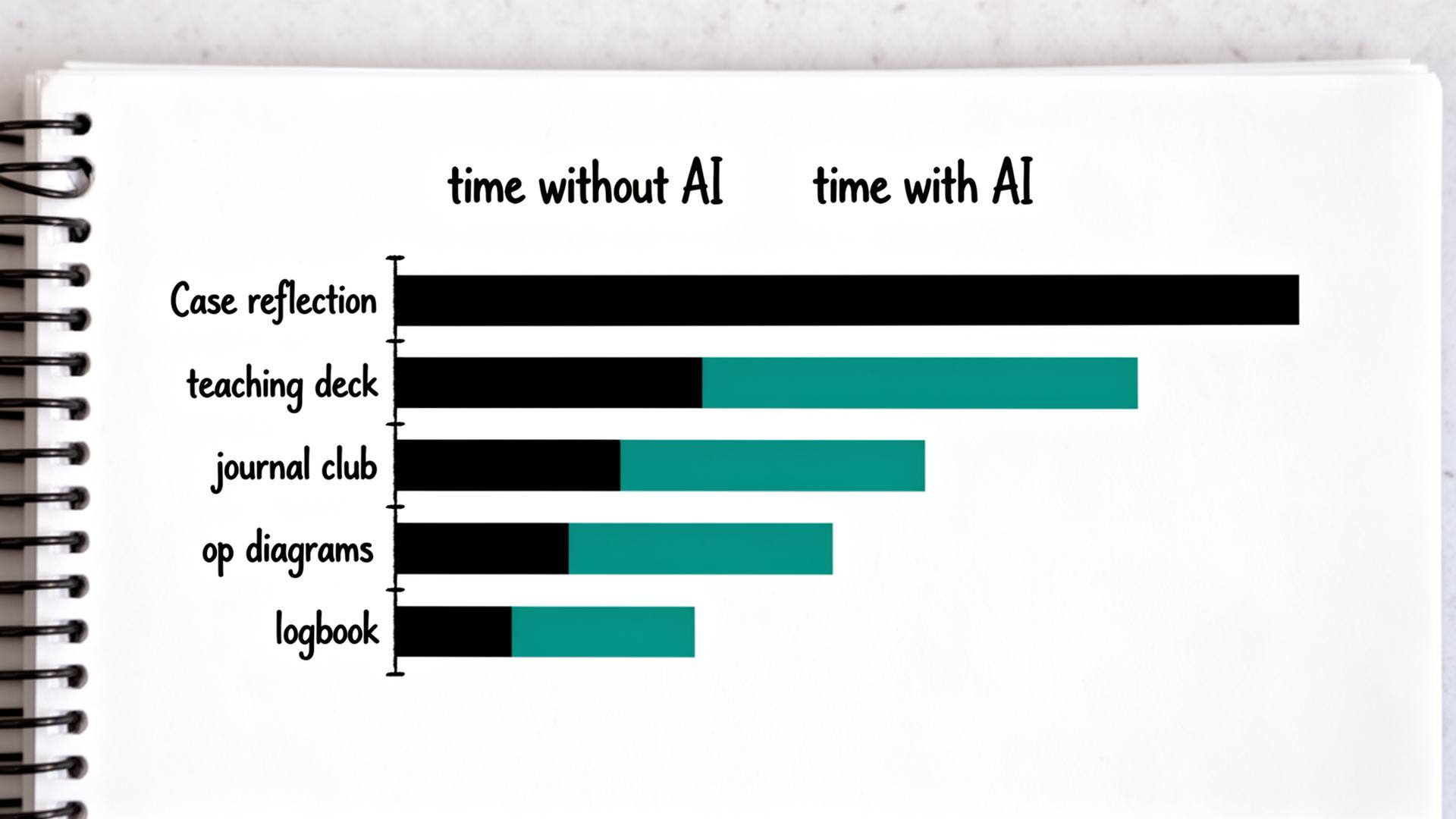
The honest time-cost vs time-saving table
Numbers below are median estimates from informal trainee surveys (UK Foundation, IMT and Core Surgical, 2024-2025). They assume you already have a clear prompt and verify the output before submission. Without verification the time saving is illusory and the clinical risk is real.
| Task | Without AI | With AI | Verification time | Net saving |
|---|---|---|---|---|
| Case reflection (200 words) | 30 min | 5 min | 5 min | ~67% |
| Teaching deck (12 slides) | 2-3 hours | 30 min | 20 min | ~70% |
| Journal-club summary | 60 min | 10 min | 10 min | ~67% |
| Operative teaching diagrams | 2 hours+ | 20 min | 5 min | ~80% |
| Logbook narratives (batch of 10) | 90 min | 15 min | 10 min | ~72% |
| Audit data review | Variable | No saving | n/a | 0% (do it yourself) |
Hard limits that protect your registration
Postgraduate training operates under a tighter regulatory frame than medical school. The four limits below are not optional and are not soft. Crossing them risks an ARCP outcome 3 or 4, a GMC referral, or a coroner's letter.
| Limit | Rule | Regulator |
|---|---|---|
| Patient identifiable data | Never paste names, MRNs, DOBs or rare features into cloud AI | GMC GMP 2024; NHS IG Framework |
| Drug doses | Always verify AI doses against BNF or local formulary before prescribing | GMC Prescribing Guidance 2024 |
| Clinical decisions | AI is a second opinion at best; you remain the accountable clinician | GMC GMP 2024; ACGME CPR 2024 |
| AI scribes on ward | Use only within an approved trust pilot with patient consent | NHS England Ambient AI Guidance 2024 |
A workable weekly stack for a trainee
- Monday on-call write-up: bullet the cases on the train home, paste into ChatGPT with an eportfolio prompt, edit on arrival, sign.
- Tuesday teaching session: outline 10 bullets, drop into Gamma, replace stock images with Radiopaedia or sketch-first diagrams, present.
- Wednesday journal club: load paper into NotebookLM, generate PICO summary, draft three critique questions, cross-check against the paper.
- Thursday operative teaching: sketch each step on an iPad, render with Angiosome, assemble into a one-page teaching aid for SHOs.
- Friday revision: Anki review, then 20 minutes of viva rehearsal with Claude playing the examiner.
AI scribes, ambient documentation and what is actually live in the NHS
Ambient AI scribes (Abridge, Heidi Health, Nuance DAX Copilot, Tortus, Nabla) are appearing in NHS trusts and US health systems through 2025 and 2026. The 2024 NEJM Catalyst evaluation by Tierney and colleagues of an ambient scribe across 3,442 Permanente physicians reported a fall in documentation burden and a modest rise in patient-facing time, with high physician satisfaction. The evidence for nursing and junior doctor cohorts is thinner.
Practical rule: only use a scribe inside an approved trust or department pilot, with patient consent recorded in the notes, and only sign documentation you have read in full. NHS England's 2024 ambient AI guidance is explicit that the clinician remains the author of record regardless of who or what generated the draft.
What AI does not help with in training
- Procedural skill. No model replaces deliberate practice under supervision; the only way to learn a chest drain is to insert one with a senior watching.
- Clinical judgement under uncertainty. AI hedges in ways patients cannot. The model never has to call the family at midnight.
- Breaking bad news and ethical conversations. The model has read every textbook on SPIKES; it cannot have the conversation.
- Audit data collection. AI summarises columns you give it; it will not chart-review the notes for you.
- Calibration against real exam questions. AI explanations are good; AI question generation is currently below the standard of dedicated banks.
Sources
- Tierney AA et al. — Ambient AI scribes and physician documentation (NEJM Catalyst, 2024)
- GMC — Good Medical Practice (2024 update)
- GMC — Good practice in prescribing and managing medicines and devices (2024)
- ACGME — Common Program Requirements (2024)
- NHS England — Ambient voice technology and AI scribes guidance (2024)
- BNF — British National Formulary
- Google — NotebookLM product page and context limits
- JCST — Surgical training and digital portfolio guidance
Frequently asked questions
What is the best AI tool for registrars and residents in 2026?
ChatGPT (GPT-5) and Claude Sonnet 4.5 are the strongest general models, NotebookLM is best for source-grounded paper and guideline work, Gamma is fastest for teaching slides, and a sketch-first tool such as Angiosome is the only safe option for operative and anatomy diagrams. The combination beats any single tool.
How much do AI tools cost for a junior doctor?
Most trainees get through a full training year on free tiers of ChatGPT, Claude, NotebookLM and Gamma, plus free Anki. Paid tiers cost roughly £16/month for ChatGPT Plus and £15/month for Claude Pro; trainees writing reflections daily often find one of them worth it, but stacking three subscriptions rarely is.
Is AI safe for clinical decision-making in training?
AI is a second opinion at best, never a first one. The GMC's 2024 Good Medical Practice update keeps the trainee as the accountable clinician regardless of which tool drafted what. Use AI to challenge your reasoning, broaden a differential, or check a guideline reference; never let it override a senior or replace a discussion with one.
Can AI write my eportfolio reflections without breaching ARCP rules?
Yes, if you personally edit, verify and sign every entry. UK royal colleges and the JCST accept AI-drafted reflective prose at ARCP from 2025 onwards, provided the content is accurate, identifiers are removed and the reflection genuinely represents the trainee's thinking. Submitting unedited AI text is treated as probity failure and can trigger an ARCP outcome 3.
Can I use AI scribes like Tortus or DAX on the ward?
Only inside an approved trust or department pilot, with documented patient consent and a clear local information governance sign-off. NHS England's 2024 ambient AI guidance treats unsanctioned use as an IG breach. Even within a pilot, the clinician remains the author of record and must read every line before signing.
Will AI replace junior doctors?
No, and the evidence so far points the other way. The 2024 NEJM Catalyst Permanente study showed AI scribes reduced documentation time and increased patient-facing time without reducing physician headcount. AI changes what junior doctors spend their hours on; supervised practice, judgement under uncertainty and team communication remain irreducibly human.
Can my training programme detect AI-written reflections?
Turnitin's AI detector and similar tools are imperfect but increasingly used by deaneries and US residency programmes. Raw, unedited AI text is detectable about 60 to 80 percent of the time in academic settings (Walters and Wilder, 2023). AI used to draft a structure that you rewrite in your own voice is both legitimate and undetectable; it is also what most regulators now expect.
What is the best AI workflow for journal club as a registrar?
Load the paper into NotebookLM, ask for PICO, primary outcome, secondary outcomes, key limitations and the strongest critique. Verify each claim against the paper. Use ChatGPT or Claude to rehearse three challenge questions you expect from consultants. Total prep time falls from about an hour to roughly 15 minutes, and you arrive with a clearer argument than from skim-reading alone.
Try it
Sketch it. Angiosome renders it.
Angiosome turns rough medical sketches into clean, labelled, photoreal diagrams — grounded in your sketch, not invented by a model. Free to try.
Open Angiosome →Keep reading
Pillar
AI for Medical Students: 2026 Playbook
Pillar
Best AI Tools for Medical School (2026, Ranked)
Pillar
AI Medical Illustration: The Honest Guide (2026)
How-to
How to Make Medical Diagrams with AI (2026)
Tool deep-dive
AI Presentations for Medical School: 2026 Guide
Tool deep-dive
NotebookLM for Medical School: 2026 Guide
Audience
AI for Medical Educators: Teach More, Mark Less